

A Practical Case Against Vaccine Mandates
A Practical Case Against Vaccine Mandates
Bolstering the defense of medical freedom

Previously, I argued that medical mandates are unethical. No society should force anyone to use a medical product such as a vaccine or a medical mask against their will. I did not argue that it is unethical or unjust for individuals to impose a medical requirement on their private property, or for individuals to shame their peers for not taking a vaccine. Society should not impose laws on what people choose to do in their private lives.
There is, however, a case to be made that, save for a few exceptions, it is impractical to discriminate against people based on their refusal to use certain medical products.
In this article, I will focus on vaccines.
Vaccines are overrated
First and perhaps most important to understand is that the role of vaccines in eliminating disease is overstated. Our forbears succumbed to all sorts of diseases which no longer pose much of a threat in developed countries. Some of those diseases can be treated today with vaccines while others disappeared as a result of advances in medicine, nutrition, and sanitation.
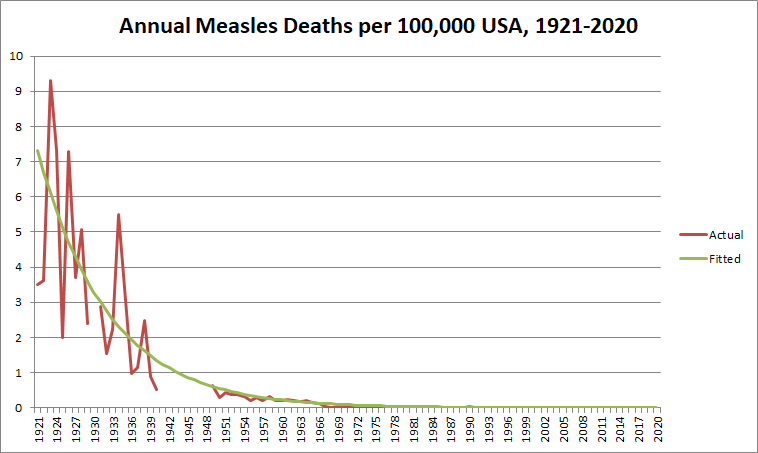
Vaccines are usually touted as the main reason for the reduced spread of certain deadly diseases, but deaths from disease have been in decline since the early 1900’s, decades before the first vaccines became available.
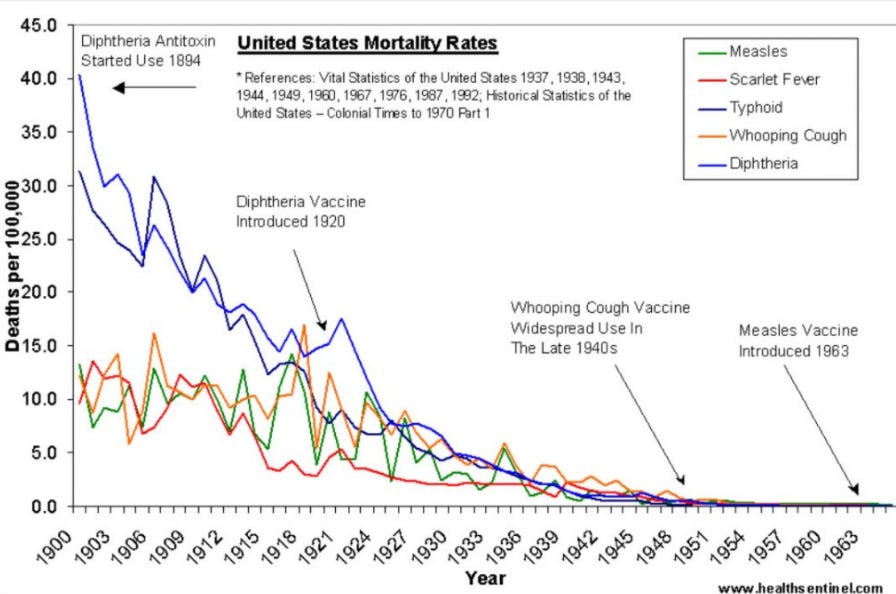
If we were to extrapolate the pre-vaccine mortality rates for these diseases till 2022, the predicted deaths in the U.S. from these diseases even without a vaccine would be minimal. Doing this for measles results in an estimated 3 measles deaths in 2020 without a vaccine. Though the actual number of annual measles deaths would likely be a bit higher, the point of the extrapolation is to illustrate that even if many people did not get vaccines, there would likely be very few deaths from diseases like measles.
Because modern, industrialized societies tend to reduce the harm of infectious diseases even in the absence of a vaccine, it makes very little sense to stigmatize people who choose not to get vaccinated. Vaccines target diseases that pose a minimal threat to populations in developed nations. Therefore, unvaccinated people also pose a minimal threat to their neighbors and family if they refuse vaccination.
Vaccine Induced Herd Immunity
A second argument for vaccine mandates revolves around vaccine-induced herd immunity. There are some people who are not able to get vaccinated, such as infants or the immunocompromised. In order to protect these people, a population needs to achieve herd immunity. The herd immunity threshold is the minimum percentage of the population that needs to be immune in order to keep a disease from exponentially spreading.
In order for a population to reach herd immunity with vaccines, a certain percentage of people need to be vaccinated. The percentage is the ratio of the herd immunity threshold and the effectiveness of the vaccine.

For example, if a disease has a a herd immunity threshold of 70%, and a vaccine is 70% effective in stopping transmission, then 100% of the population needs to be vaccinated to reach herd immunity. If the herd immunity threshold is 50% and the effectiveness of the vaccine is 90%, then 56% of the population needs to be vaccinated to reach herd immunity. If the herd immunity threshold is higher than the effectiveness of the vaccine, then it is impossible to reach herd immunity with a vaccine.
Vaccine-induced herd immunity is commonly used as a reason to mandate vaccination. But it’s important to remember that the herd immunity argument can only justify mandating a narrow selection of vaccines.
Herd immunity does not result in the elimination of a disease. It only prevents the exponential spread of a disease. Herd immunity reduces the likelihood of catching the disease at any given time, but it does not guarantee a reduction in the chance of catching the disease over a lifetime.
Only highly effective vaccines can significantly reduce that risk. Even then, there is still a chance of the unvaccinated getting the disease.
Probably the strongest practical case to be made for vaccine requirements or discrimination is for the measles vaccine. Measles is highly contagious, has slow genetic drift, is particularly dangerous for infants who cannot get vaccinated, and has a very effective vaccine. Certain employers may want to require a record of immunization as a prerequisite for employment. New mothers may want to be particularly cautious about who their young children interact with.
For many other diseases, the same herd immunity argument for vaccine mandates or discrimination cannot be made.
With COVID-19, vaccine-induced herd immunity was theoretically improbable from the get go. At the start of the vaccine campaign in 2021, COVID-19 purportedly had a herd immunity threshold of around 60-70% and we knew it had a fairly rapid genetic drift just like all other coronaviruses. That meant that even if herd immunity were to be reached through natural infection, future reinfection would be very probable due to future variants The shots were not tested for transmission prevention in the clinical trials, so there was no way to know just how effective they were really were. Now, a year and a half later, it is clear to anyone who is not in denial that these shots were not very effective at all in preventing transmission.
The mandates and discrimination therefore made very little sense. Without a known effectiveness against transmissibility, it was impossible to know how many people would even need to be vaccinated in order to reach herd immunity. Only a highly effective vaccine could even have a chance of getting a population towards herd immunity, and this is practically impossible to do against diseases with rapid genetic drift. Add on top of that the logistical challenges of vaccinating an entire population to achieve herd immunity and the unknown risks of mass vaccination (ADE, vaccine evasion, OAS) and the mandates seem even less reasonable.
Now looking back, we see how pointless the mandates and discrimination actually were. Many people who got the jabs have since tested positive for COVID-19 and gotten very sick. Countries with high rates of vaccine uptake never reached herd immunity because of the vaccines.
The lesson from the past year and a half is not that we need to “try harder”, develop “better” vaccines, or implement stricter mandates. The lesson is that it is practically impossible to reach herd immunity through a mass vaccination program in a short amount of time, regardless of the disease.
Risks of Vaccination
Herd immunity is desirable because it protects those who are not able to get a vaccine. This is, however, a tacit admission that vaccines are not risk free for anyone. Even though the risks are low for many people, there is still some risk.
Who then determines whether individuals ought to get vaccinated because the benefits outweigh the risks? Is it the doctor who sees their patients a couple times a year? Is it the bureaucrat sitting in an office hundreds of miles away? Or should it be the individuals themselves? What is the risk threshold that determines whether a person ought to be vaccinated, and who determines this risk threshold?
Risk is a part of any medication or medical procedure, and people ought to be able to make their own decisions based on their knowledge of the risks and benefits.
Critics of parents who do not vaccinate their children accuse those parents of selfish free-riding. The children are not exposed to the risks of vaccination but enjoy all the benefits of herd immunity when everyone else is vaccinated. I’m not sure how many people are actually conscious free-riders, but I certainly don’t know of any. Most parents I am aware of who choose not to vaccinate their children are concerned with the potential negative side effects of vaccination. There is debate about whether these concerns are scientifically sound, but that is not the point. Parents are concerned about risks, sometimes they see the negative side-effects take place in children, and they refuse to get their children vaccinated.
Again, the fact that certain people cannot get vaccinated due to the risks, and therefore everyone else needs to get vaccinated to protect those people, is a tacit admission that there is enough risk for certain people to not get vaccinated. This justifies many people’s concern with vaccinations, in case for some yet unknown reason they happen to be that person who should not get vaccinated.
People get vaccinated anyways
In Switzerland, vaccinations are not mandatory, even for public schools. Despite this, MMR vaccination rates for children are around 96%. The same is true for Sweden. Even though the government does not force usage of the MMR vaccine, parents voluntarily decide to vaccinate their children with the MMR vaccine.
If medical experts establish trust with the populace, then people are more likely to do what medical experts think is best for the population. The overwhelming majority of people perceive that the benefits of vaccination outweigh the risks, so they choose to vaccinate their children.
This underscores the principle that trust and a quality product or more effective than force and make government mandates impractical. Coercion sows distrust, skepticism, and resistance. If people wish for their friends and family to get vaccinated for certain disease, the best way to do so is through persuasion.
None of this is to argue whether people should or should not get vaccinated. Indeed, certain vaccines have shown to eliminate the target disease when a significant proportion of the population is vaccinated. However, coercing people to take a vaccine is not only unethical, but impractical. Without vaccine mandates, most people get vaccinated anyways. The diseases themselves do not pose a significant risk to society at large. Finally, every medical intervention comes with a risk. People should be able to decide for themselves whether the benefit of not getting sick is worth the potential risks.